














- Military
- Security & Defense
- History
- Determining America's Role in the World
The author, Professor of Surgery at the Perlman School of Medicine at the University of Pennsylvania, is a Veteran Fellow in Hoover’s Bochnowski Family Veteran Fellowship Program for 2024–25. He served on active duty in the US Air Force from 2006 to 2015 and deployed to both Iraq and Afghanistan as a trauma surgeon during that time. In 2023, he retired as a colonel from the US Air Force Reserve.
“Medical care is no longer just a secondary consideration. In the current age, it has become and should remain an integral part of military strategy.”—Victor Davis Hanson
In his classic film The Seventh Seal, Ingmar Bergman portrays a knight engaging death in a game of sudden-death chess. Like that intrepid knight, medical practitioners over millennia have sought to offer their armies a strategic advantage by warding off death from injuries, contagion, and disease. With the writings and insights of Hoover senior fellow Victor Davis Hanson as a backdrop, this essay explores the historical evolution of the means used to outmaneuver death on the battlefield. These lessons point to the importance of leveraging medical knowledge and innovations to overmatch one’s enemies, including the ultimate enemy: death.
Yet, in the face of peer enemies in the current geopolitical climate, our Military Health System now stands in critical disrepair, having gradually slid into obsolescence over the past decade. Depleted ranks of military trauma experts, lack of leadership support and infrastructure for trauma training, and reduced funding for injury-related research have all contributed, as I testified in March before the Senate Armed Services Committee. At present, only 10 percent of military general surgeons are combat ready. Urgent attention to such deficiencies is needed to ensure our service members do not needlessly suffer the fate of Bergman’s knight.
To win in future conflicts, the United States must treat battlefield medical care not as an afterthought but as a foundational strategic priority. What does this mean in a modern context? Advances in sanitation, nutrition, and environmental protection have largely neutralized many of the most infamous historical threats to the fighting force that I explore here. Thus, outmaneuvering death now centers principally on both injury prevention and expert trauma management from the point of injury to definitive care.
Ancient warfare and early battlefield medicine
As Victor Davis Hanson explains, “Studies on Greek classical warfare in Xenophon, Thucydides, and Herodotus reveal that the winning side usually lost about 5 percent of their soldiers and the losing about 15 percent.” In the Iliad, we find descriptions of death occurring most often from penetrating wounds from spears, arrows, and swords, mostly during single-champion battles. Blunt-force trauma from stones and other implements represented a much smaller proportion of injuries.
During set-piece hoplite (infantry) wars between city-states, defensive weapons and personal armor made of bronze with leather padding proved very effective at defending against penetrating wounds. Shields afforded excellent protection against spears and arrows for both the bearer and the adjacent hoplite. Helmets covered the entire face, including the nose and cheeks. The breastplate could turn arrows except at very close range. Soldiers’ groins were protected by very thick leather strips called pteruges that afforded protection without limiting mobility. Greaves went from the knees to the dorsum of the foot. Thus, as Hanson writes in The Western Way of War, with all this protective equipment, the most common deaths were from suffocation or trampling within the ranks of the phalanx, or from spear wounds to the back.
For wounded survivors, the earliest recorded therapies come from Hippocrates, representing a school of thought rather than an individual. These included application of honey or sugar to soft-tissue wounds. For major head injuries, Hippocrates and later Galen employed trephination, a procedure where a hole is drilled in the skull to relieve intracranial pressure. All these ancient approaches have modern analogues, including MediHoney for wounds and decompressive neurosurgical procedures.
Campaign warfare
As weapons evolved, the risk of fatal injury increased. The siege of Constantinople in 1453, as described in The End of Everything, illustrates this well. Quoting Hanson again, “For a thousand years, nobody had ever gone over the Theodosian Walls. They were kind of a death trap for anybody who tried.” Yet when Mehmed II attacked, cannon reduced sections of the walls to rubble, while the arquebus and improved crossbows with a steel frame increased mortality when they struck defending soldiers.
Along a key section of the wall, the brilliant Genoese leader Giovanni Giustiniani Longo and his seven hundred men held strong for months until a projectile from one of these new weapons struck the commander. Giustiniani ordered his men to remove him from the wall, thinking the fighting would continue. With their superior galleys, the Genoese slipped through the Ottoman blockade with Giustiniani aboard and escaped to the island of Chios, hoping he might survive. Nevertheless, Giustiniani died within a few days, the city fell, and according to Hanson, debate over his legacy continues: “Today, when you read the Greek sources, some talk about Giustiniani as a coward or a traitor because the city fell soon after his men evacuated him. When you read the Italian sources, though, they describe him as a wonderful protostrator, a famous condottiere.”
As battles moved from set pieces to protracted campaigns, the threats to life among armies shifted as well. Although physical injuries remained a serious risk, contagion, disease, nutrition, and environmental factors played an increasingly important role. Diseases, poorly understood and often mismanaged, including malaria, typhus, and dysentery, and they spread quickly within the military ranks, sometimes disabling entire units. During the Hundred Years War, outbreaks of the bubonic plague or “black death” halted combat operations for years at a time. Near the end of the war, on the eve of the 1415 Battle of Agincourt, a lethal outbreak of dysentery among Henry V’s troops threatened to neutralize their advantage over the French.
Environmental exposure, including extreme cold and punishing heat, also disrupted campaigns, most famously the Napoleonic invasion of Russia in 1812. Finally, invading armies disrupted fragile ecosystems for local populations. In their wake, food shortages and disease outbreaks often followed, leading to large death tolls among civilians.
Warfare in the New World
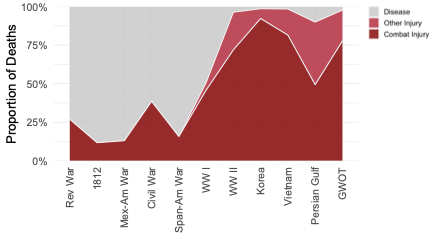
This constellation of diseases, environmental factors, and injuries manifested abundantly in New World conflicts as well. The relative contribution of these factors to death rates in each major US conflict is shown in the following chart.
(GWOT, Global War on Terror; Mex-Am, Mexican-American War; Rev War, Revolutionary War; Span-Am, Spanish-American War)
In the American Revolution, the celebrated patriot and physician Joseph Warren died in the Battle of Bunker Hill in 1775 from a gunshot wound to the head, while Benedict Arnold and the Marquis de Lafayette cheated death after serious injuries to the leg. Combat wounds were far less costly to the Continental Army than a host of diseases including smallpox, malaria, typhoid, and environmental exposure, including heat exhaustion and frostbite.
A smallpox outbreak contributed to the Continentals’ failed attack on Quebec, eventually leading General George Washington to mandate inoculation in the Army, a risky and highly controversial practice. This medical decision served to preserve the American fighting force, thus neutralizing the advantage of relative immunity held by the British.
During the Civil War, the Union Army held a strategic advantage in terms of medical care, partly because the pre-eminent medical schools such as Harvard and Yale were in the North. The importance of preventative medicine and sanitation also emerged during this conflict. The North used rubberized ponchos that appeared to reduce rates of pneumonia. Latrine placement downstream or away from drinking-water sources decreased dysentery. And for surgeons, one old idea—that respect was earned by the layers of crusted blood on one’s clothing—no longer held. Physicians also started to recognize empirically the value of clean hands and of cleansing the wound as practiced by Hippocrates.
For extremity wounds, the standard treatment became application of a tourniquet.
Although the use of tourniquets doubtless saved many lives, amputation often followed. As one famous event demonstrates, though, the initial wound had to be identified as life-threatening before it was too late.
In April 1862 at Shiloh Church, Southern field commander Albert Sidney Johnston led a successful charge against Ulysses Grant’s larger Union force. When Johnston returned from the charge, he felt faint and confessed, “I am hit, and I fear seriously.”
Johnston’s aide thought he had fainted or had a heart attack, but as blood started pouring out of his riding boot, the diagnosis became clear: a bullet had transected his popliteal artery right behind his knee. Tragically, after his death Johnston was found to have a tourniquet in his uniform coat pocket; properly applied, he would have lived. The loss of this charismatic, beloved figure helped create the greater myth of the Southern “lost cause.”
The world wars
Mechanized warfare greatly increased the number and proportion of battlefield deaths from combat injuries, accidental discharges, airplane crashes, and the like. Yet disease did not disappear from the battle fronts and training camps. The highly lethal influenza pandemic of 1918, for instance, greatly eroded US fighting strength in World War I.
As offensive weapons evolved, so too did defensive approaches that served to cheat death and neutralize any strategic advantage. The Germans first developed phosphene and chlorine gas, which they used in 1915. But by the time they started using mustard gas regularly in 1917, the French and the British had developed advanced rubber gas masks that rendered these horrific agents ineffective.
The need for rubber resurfaced in World War II in other ways that affected service members’ health. As discussed by Hanson in The Second World Wars, when the Japanese took Singapore in 1942, they suddenly controlled the world’s most plentiful supply of rubber. The Americans were worried they would lose access to essentials like rubber tubing, bottle stoppers, absorbent rubber, and cleaning implements for medical units, not to mention tires. In response, Goodrich, Armstrong, and other American companies produced synthetic rubber en masse, and by late 1943, the Allies had an abundance of rubber that gave them a major advantage.
Antibiotics also afforded a strategic advantage in World War II, serving to limit the number of fatal infections. Winston Churchill was a beneficiary—he contracted pneumonia en route to his 1943 meeting with General Dwight Eisenhower in Carthage, Tunisia. Churchill, exhausted, had a fever of 102 degrees and was short of breath. His physician gave him sulfa antibiotics in the villa where he lay in bed, with seemingly miraculous results. By then, the tide had turned for the British and Americans, in part because they had better health care than Axis forces late in the war. The mass production of penicillin helped tip the scales. However, “casualties of the brothels” suffering from sexually transmitted diseases diverted vital resources from those with actual combat wounds, thus eroding the strategic benefit of this innovation.
Protective equipment also played an important role, although, according to Hanson, the Axis powers held the advantage there. “The more extensive German helmet, which our current American helmet is modeled after, reduced head and neck wounds by 30 percent compared to their British and American counterparts. So why did the Allies all have such different helmets? Making helmets like the Germans, regardless of the superior design, was considered imitative or perhaps confusing in battle.” In a similarly curious evolution, early flak vests were primarily used by air crews rather than ground troops, as the weight and bulk of early designs tipped the balance in favor of exposure to enemy bullets over restricted mobility or potential heat stroke.
Medical supremacy on future battlefields
Innovations in battlefield trauma care in Korea and Vietnam included rapid helicopter transport of those with combat injuries to Mobile Army Surgical Hospital (MASH) units. Severely injured patients were managed for the first time with dialysis and mechanical ventilators in combat hospitals on the battlefield. Preventive measures including insect repellent, mosquito nets, and malaria prophylaxis further reduced disease-related fatalities.
Twenty years of combat during the Global War on Terror (GWOT) built upon these tools to outmaneuver death. Advanced body armor and stylish eye protection that combined form and function increased compliance, saving the lives and eyesight of many. Those who suffered injuries benefited from a trio of life-saving “golden hour” interventions: tourniquet application for extremity wounds, blood transfusion, and rapid evacuation to a surgical unit.
In the face of a determined adversary, US combat units need superior medical technology, expert trauma team training, and operational freedom of movement to win the day. Achieving and sustaining these advantages in a life-and-death struggle requires deliberate effort. Failure to pursue medical supremacy with urgency risks a chilling outcome: checkmate.

